
This Lancet study published on 5th April 2017 (http://thelancet.com/journals/lancet/article/PIIS0140-6736(17)30819-X/fulltext) systematically analysed almost 3000 data sources across 195 countries between 1990 and 2015 to demonstrate comprehensively that smoking is still one of the main killers worldwide. This huge undertaking was possible owing to a large Global Collaborator Network which the Institute of Health Evaluation and Metrics (IHME) have managed to co-ordinate and execute.
I am one of the GBD collaborators from Ireland to have contributed to this Lancet study. So, why now when a similar study was published in 2013?
Firstly, with the 2015 update to the GBD study, a number of new data sources were included and the estimates were thus improved. Secondly, a new summary measure of overall development of a country- the Socio-Demographic Index (SDI) was used to assess levels and trends in smoking prevalence and attributable burden across the development spectrum. Finally, two novel analyses were provided: a birth cohort analysis of smoking patterns over time and a decomposition analysis to parse out changes in total DALYs attributable to smoking to changes in population growth, population ageing, smoking prevalence, and risk-deleted DALY rates.
What are the main findings then?
In 2015 worldwide, the age-standardised prevalence of daily smoking was 25% (95% uncertainty interval [UI] 24·2–25·7) in men and 5·4% (5·1–5·7) in women. Smoking was ranked among the five leading risk factors by DALYs in 109 countries and territories in 2015, rising from 88 geographies in 1990. About 51 countries and territories had higher prevalence of smoking than the global for men. These countries were mainly located in central and eastern Europe and Southeast Asia. About 70 countries and territories had higher prevalence of smoking than the global for women and they were mainly in western and central Europe. Prevalence of daily smoking in men was highest in middle SDI countries whereas for women it was in high SDI countries. There was a sharp decline in the global age-standardised prevalence of smoking for both sexes, declined by 28.4% in males and 34.4% in females. 13 countries (Australia, Brazil, China, Denmark, Dominican Republic, Iceland, Kenya, the Netherlands, New Zealand, Norway, Sweden, Switzerland, and the USA) recorded significant annualised rates of decline both between 1990 and 2005 and 2005 and 2015, suggesting sustained progress in tobacco control.
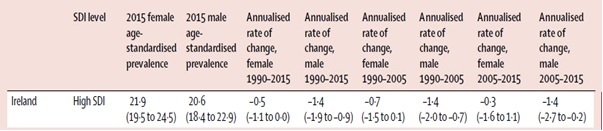
The Irish scenario of smoking prevalence across both genders, annual rate of change in prevalence between 1990 and 2015 and also between 1990 and 2005 for both genders are provided in the table below. There has been declines in the prevalence of smoking in Ireland across both time periods 1990-2005 and 1990-2015 for both genders.
Despite efforts to control tobacco around the world, there are a number of countries where current levels and trends raises concern. The countries are: Indonesia, Russia, China and India. As a region, Eastern Europe has seen a statistically significant increase in smoking prevalence among women since 1990.
In summary, there have been some success stories, but for many countries and territories, faster annualised rates of decline in smoking prevalence occurred between 1990 and 2005 than between 2005 and 2015. Although smoking prevalence and risk-deleted DALY rates fell across SDI quintiles, population growth and ageing ultimately offset these gains and contributed to overall increases in smoking-attributable disease burden in low to middle SDI geographies.
Future directions?
Well, the ongoing GBD study will focus on other nicotine products, such as smokeless tobacco products and electronic cigarettes, as well as to map the disease burden attributable to secondhand smoke exposure which were not considered in the current Lancet paper. Moreover, such future GBD studies will help monitor progress in tobacco control across countries and territories where new anti-smoking interventions have been introduced in alignment with the WHO Framework Convention on Tobacco Control. One such example will be standardized packaging of cigarette packs. More recently, WHO introduced the 25×25 non-communicable disease (NCD) targets, which include decreasing tobacco use by 30% between 2010 and 2025. With tobacco control’s increasing prioritisation on the global stage, accurately monitoring patterns in smoking and associated health outcomes is critical for identifying optimal intervention strategies across geographies, demographic groups, and the development spectrum. The GBD studies will help provide solutions to these questions.
Dr. Zubair Kabir,
Department of Epidemiology and Public Health,
University College Cork
If you have any questions or comments please contact Martin on m.davoren@ucc.ie